How to get Digital Health into the Health Care Curriculum: A framework model with pharmacy schools as a case example

Well, I guess it's time to take a crack at trying to create a theoretical framework of how I would introduce digital health into the curriculum. Look, I've been a pharmacy professor for almost a decade, so that's my bread and butter and what I am going to use as a case example - but I have no reason this same approach couldn't be approached by other health schools (e.g., PA, NP, MD/DO, nursing).
So if you are interested to see the approach, read along. I think this will be beneficial for several groups:
For those that are academically focused, this might help get you thinking of how to role digital health content out in your programs.
If you are in the industry, a digital health-focused company, etc., this will still be of interest as it's your products and services that the next generation of practitioners are going to use, so you probably want to consider how we'll go about educating them on how to use your stuff. How will you align CEs and other training modalities into your marketing and commercial strategies will eventually come up. After all, getting FDA clearance is only the halfway point of getting the product to the market.
Now, this is following after a previous post of mine about current digital health offerings we are seeing and a publication by Ravi Patel and myself that thought about how to get digital health into the curriculum. This builds upon those offerings and offers a more theoretical model of actually doing something beyond a 101 or introductory course but actually breaking digital health into the formal curriculum. So let's get into it.
What Do We Teach In Pharmacy School?
I think the first place to start is considering the pathway of educating students. So to begin with, you have your prereqs before coming to school. Same with any other health professional. Pharmacy focuses on the human body (A&P) and chemistry (Medications, right?), with odds and ends (e.g., physics, English, calc).

This is not necessarily a complete model of how pharmacy schools teach content but represents some overarching topic areas and their relationship. Pharmacy sciences do not hate me plz.
Well, get into pharmacy school, and then there are some different levels. On the one hand, you have the pharmaceutical sciences and pharmacy practice departments (and some others, depending on the program focus). The sciences focus on things like what is the molecular action of a medication and how it reacts on the receptor and impact on the body, for instance. How does an organ system work and what problems (i.e., diseases) may come about. Pharmacy practice takes this scientific knowledge and can apply it to items like how to deliver pharmaceutical care, such as what are best practices/guidelines for disease management, which medication works in what situation and why, and related aspects of pharmacy practice. One of the high-level courses then in pharmacy school is pharmacotherapy, which fixates on this topic, usually by a systems-based approach. So, for instance, you get cardiology, pulmonology, endocrinology, etc. Then you start thinking, how do you manage hypertension, for instance? That builds upon all the pharmacology of medications, pathophysiology, and related sciences. So that's the quick overview, and I know it varies and that this may not do it justice, but we're not here to do a full-on breakdown of the whole curriculum.
Why Can't We Just Throw In Digital Health Material?
Now, why do we decide to teach this is a good question. There are items like accreditation which relies on schools to teach certain topics based on educational standards. So for us in Pharmacy, we got things like ACPE, CAPE, EPAs, and more to think about. The courses and topics try to address and assess all of these items. The bottom line is to then consider that educators and institutions how an MVP to teach, and that is all based on the curriculum timeline. So if you want to add material, then what do you remove? How does that impact anything else? These things need to be considered.

Bottom Line: WHERE DO WE FIT THIS IN?!
Because, at the end of the day, if we are talking about putting digital health into the curriculum, then we need to be thinking about what that does to the current courses and what could be upset. There's other items to consider too. Have you been in a faculty meeting where people are arguing to remove someone's course or lectures? It's not pretty. Thinking about all the time they dedicated towards that material, and you want them to just throw it away? There's a reason we get terms like 'curriculum hoarding.' Also, do you have people that can teach new topics, or how are you going to get up to speed with new topics? Not every academic is an expert in XYZ. Taking this all into consideration is going to impact this theoretical model going forward. Otherwise, it just won't fit or would be a mess because it doesn't mesh with anything else going on in the student's curriculum. And trust me, students hate when things don't go together.
One Second, How Difficult is it to Just Teach Digital Health Then?
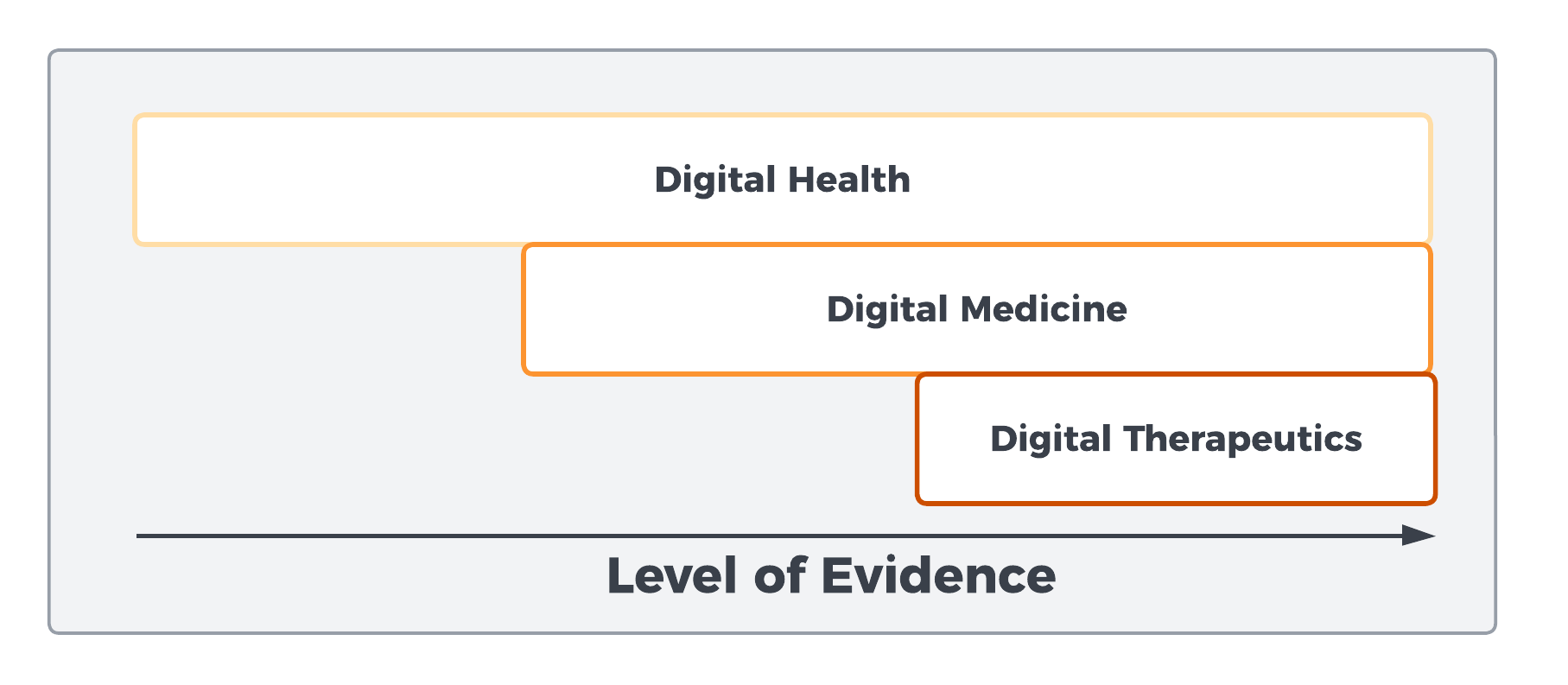
Debatable but my overarching thought process of digital health as an umbrella term with different arching levels of evidence for certain types of innovations.
Well, that depends, I think. If we accept that digital health is an evidence-based subject in the realm of healthcare, then I think it deserves a higher level of understanding. It's not just saying, let's digitalize patient care pathways, like engaging in telehealth and changing in-person to remote and saying, let's just add webside manners and wash our hands of it. No, if we start adding on and treating areas of digital health like digital biomarkers as a means of conducting disease diagnosis and guiding management, and that some therapies are at the level of current medical therapies, then I see no reason to accept to understand the scientific basis of how those principles work.
But that is a problem. We'd have to then determine what do we need to know and include. For instance, and I'll be using medication analogies a lot going forward (remember, pharmacist), what is the level of understanding between supplements and FDA-approved medications? Could the same analogy be made between the 300,000 health-related apps (Supplements) versus the [currently] minor subset of digital therapeutics (DTx)?
For instance, if you asked me how to diabetes, I could do a pretty good job based on my knowledge and training, and practice experience. But all that is based upon really focusing on my pharmaceutical knowledge as well. Ask me about SGLT2s, GLP-1 agonists, insulin etc. I've got the scientific knowledge about the treatment and a good understanding of treatment pathways, and I keep up with the guidelines. This is all because my training set me up for lifelong learning to be prepared to deal with new concepts and ideas surrounding pharmaceutical care. Yeah, interferon was the treatment of choice for hepatitis when I was a student, but things came along as my sciences professors had indicated, so I was ready to adapt and understand new therapies.
Now start asking me about a digital biomarker utilizing wearable data to predict a patient transitioning to diabetes type 2 or how a closed-loop system works and CGM integration... well then we got some problems. We don't have the underlying scientific knowledge on these concepts currently built in, I would argue.
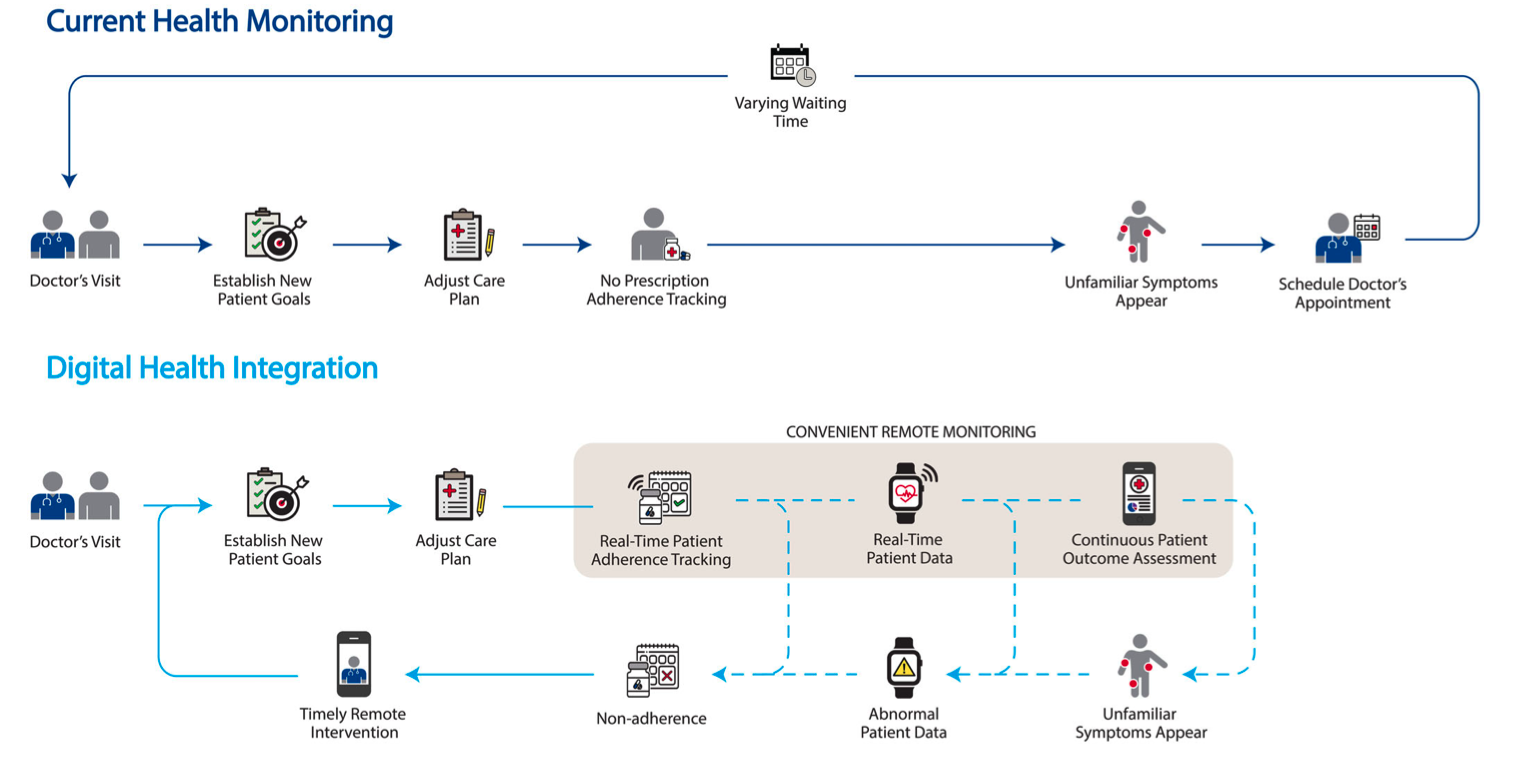
We are moving from expecting patients to show up on our timeline for intermittent visits of assessment to continuous data collection and management due to digital health.
The issue here is that these technological advances will dictate how pharmaceutical care will be delivered. I don't see them as standalone issues but now building upon them. Pharma is using digital medicine to help lead new siteless clinical trials, and if our next landmark studies in JAMA and NEJM, for instance, have a section in their methodology outlining an AI/ML algorithm that was used to guide care, shouldn't I have some knowledge of that? We train on evidence-based medicine (EBM), and if digital medicine will help guide new evidence generation and real-world evidence surrounding the use of treatments, we will need to keep updated on that at least.
So my premise is that simpling telling our students that yes, there are digital biomarkers for XYZ or new digital therapeutics for condition X isn't enough. It's just topical awareness without the underlying conceptual exploration that I think we already have built-in for our pharmacotherapy. For instance, if a DTx uses cognitive behavioral treatment as its mechanism of action, does the student even have a baseline knowledge of CBT to base it upon? If we talk about data and how it is analyzed, does a student have the ability to critique a study and highlight possible biases in an algorithm that may lead to medical misadventures?
Now, this opens up the whole gambit of where the practice of Pharmacy falls in regards to digital health, and that's a whole other topic, but if you've been reading my work, you'll know I think it's one of the areas of focus for us to increase our value in healthcare at this time.
So What Are Some Possible Models?
I've got three. I think there are probably more, but feel free to comment or add; we have that opportunity at this point. This builds upon discussions with others I've had over the years, seeing what other programs are doing, and thinking ahead on general academic politics. For instance, in Pharmacy, digital health may be an item in CAPE, which would lead to schools suddenly having to take this on (which is one of the reasons I am writing this as I think ahead).

Model A - Complete Overhaul
Some people may say, well, just add all the topics to the curriculum then. Have students have a data analytics course as a prereq. Have them code. Then when they come to school have a digital health course that introduces the topic, so when we talk about digital health treatments, it makes sense. The issue is the curriculum just doesn't have the room at this time. Even if in Pharmacy we say digital health should be taught, no one is going to redo the program to align it around that topic. It doesn't make sense.
Model B - Tracks or Curriculum Adjacent
The next model is adding a separate track that students can elect to participate in. This goes by different names, such as tracks, certificates, or focus study. This may be having your electives be focused on digital health and maybe practice experiences in rotations as well. Then when you graduate, you say you had the experience and knowledge. This can work and is what most programs seem to be adopted at this time in health care. Again, the issue is if this is an area all students need exposure to, then it becomes difficult. Maybe some level of Model C could be present in an earlier course to solve the issue and then have students elect to focus upon it much more in-depth.
Model C - Add, Subtract, and Merge
The last model is favored towards adding digital health material where available throughout the curriculum. This could include snippets here and there, perhaps a general 101 content merged into another class like US healthcare and addresses the digitalization of healthcare in the US (e.g., remote care, teleservices) or in general pharmacy profession courses as well. Once some of the foundational courses establish this stuff exists, you can add content to the clinical courses. So if you are talking about diabetes, then CGM makes sense, and you can compare and contrast care devices, talk about smart insulin pens, etc. Could do the same in others, like HTN being based upon RPM strategies and titration of care remotely and monitoring.
This model, I think, is easier for most faculty then to introduce and identify topics, speak to their role in care, and not necessarily have to be masters on digital health topics themselves. Talking pain management? Well, what about VR/MR for pain alongside traditional pharmacotherapy. Talking depression? What about digital biomarkers that can let us know how the treatment is going. Talking sleep? What DTx is available instead of medications, then. I think this could play out easier.
Theoretical Pharmacy Curriculum Model for Digital Health Integration
Ok, so you're still here. Which model do I like? Currently, I favor models B & C. I think there could be a merge between the two. However, I think Model C would be the easiest. Model B relies on having professors or partnerships with others that can really deliver the content at a level which I don't think most programs can do at this time. It might be a focus area for programs with the resources and relationships to do so. Rather, Model C, I think, could be something most programs adopt at scale.

Essentially, add where we can and where it fits.
Implementing courses to target, a few stand out to me. As I mentioned, general pharmacy practice or introductory courses are low-hanging fruit. Science classes like pathophysiology that talk about biomarkers could address digital biomarkers and novel ways of disease diagnostics. Drug Lit and biostats could also discuss digital medicines and implementation in siteless clinical trials and RWE alongside data interpretation. Pharmacotherapy could address DTx and related digital health tools available, which may include just tackling FDA cleared/approved products and others at the lecturer's convenience.

For programs thinking of taking this on in their curriculum, there will likely need to be some discussions about this. One is to leave courses to make their own decisions with the course coordinators, but I think that will probably be somewhat messy. Perhaps going on a systems-based approach will be easier. Decide on a few conditions to roll out and trial first, and maybe focus on those systems where digital health has made large in-roads. For me those are:
Cardiology with a focus on AFib, HF, HTN
Diabetes & Weight Loss
Pulmonary (COPD/Asthma)
Mental health and SMIs
Pain management
Neurology
SUDs
I think the pharmacy profession doesn't need to get bogged down with all areas of digital health at this time, and sticking with conditions that align with pharmacotherapy or adjunctive to care seems the easiest to me at this time, especially if it involves disease management. Because there's going to be some overlap ultimately between things like pharmacotherapy and surgical interventions and other psychological therapy, I acknowledge.
How to build in the content
Some items I've tried or consider that could be adapted include the following:
Do a journal club article on a digital biomarker and compare its implications compared to past or current standards of care
Do a mock P&T activity looking at a drug approval for the cost of a smart medication compared to another already on the market (e.g., smart inhaler vs traditional inhaler)
Add smart medications or devices to your medication table in a lecture similar to alternative forms of delivery
Create patient cases focused on how to act with RPM data. What if you saw on a blood pressure monitor the patient's BP was going much lower and having symptoms remotely after D/C from a hospital? How would that change your plan?
Practice doing telehealth patient communication OSCEs
Look at certain conditions and map out DTx products that may be used with or without medications. One example is looking at the recent NICE guidelines that recommend a DTx over medications or sleep hygiene for an example. Diabetes guidelines with CGM and smart insulin pens are another example.
Practice using some smart tools in labs, like how to set-up a device for a patient or how that changes patient education
Talk about data privacy and the digital health divide and how SDOH factors into all of this
Build patient cases around digital health care pathways. How does continuous data change how pharmacists could practice?
This list could be much larger, I acknowledge and may warrant another post in the future. Ultimately, you're the professor. Many faculty will find ways to add or merge content in meaningful ways over time, but sharing content and ideas will continue to help!
Advice to Faculty
So let's say you are ready and don't know where to start in terms of finding content. "Tim, where the hell do I find this information?" Well... here are some recommendations:
You could try to get some faculty to become digital health experts for your institution. I've put out some thoughts on that elsewhere.
I've put out some pieces; feel free to email me if you want the articles if you cant access them. This one probably has the largest clinical overview.
There are a bunch of digital health conferences or ones that have a focus area, like HLTH, SXSW (sometimes), HIMSS, but they can be costly. Luckily APhA is adding content, and I really thank Parisa Vantaka for spearheading this work. So just keep an eye out.
Read outside pharmacy journals. There are now many digital health-focused, such as Nature Digital Health, Sage Digital Health, etc. Many new studies are event making it to larger journals like JAMA and NEJM. The table below lists more:

Does Pharmacy really need this?
I've done enough to try to convince other academics of this. But I'll boil down some key points and leave them with you to consider:
Professional organizations are getting on board. APhA will start doing more work on this. AACP is considering a CAPE on digital health or something along that line. Professionally, we need to engage in a field other health care professions are also moving into to stay relevant.
Pharmacy as a business will be digitally focused. It's inevitable for the business, no matter what sector. So to prepare our students, this seems the time to get ahead of the ball before it drops on us too hard. We need to consider things like the "hospital-at-home" model and what that means for current health system pharmacists, how outpatient care is delivered, and what role our students will play.
How medications and next-generation therapeutics are being researched is undergoing large changes. AI, wearables, and trial design all are now in flux. How products are cleared or approved by the FDA is subject to change. The FDA launched a digital health center of excellence and is preparing for it.
New career paths are needed for pharmacists. Digital health could help our students and schools to stand apart at the end of the day. Our traditional incumbent employers are no longer enough to sustain the market.
Closing Thoughts
You may, especially if an academic, wonder why the hell did I not put this up for publication in a journal. To be honest, I know to get this across something like AJPE or CIPTL would have just taken too long. I want to move faster on this topic. So I really encourage you that if you are vested in this topic to talk more with others who are also fascinated by the topic and share ideas and concepts. If this gets people thinking that way, I think it served its purpose. I hope it helps because I know it won't be easy, but it will be worthwhile with the current environment we find ourselves within.